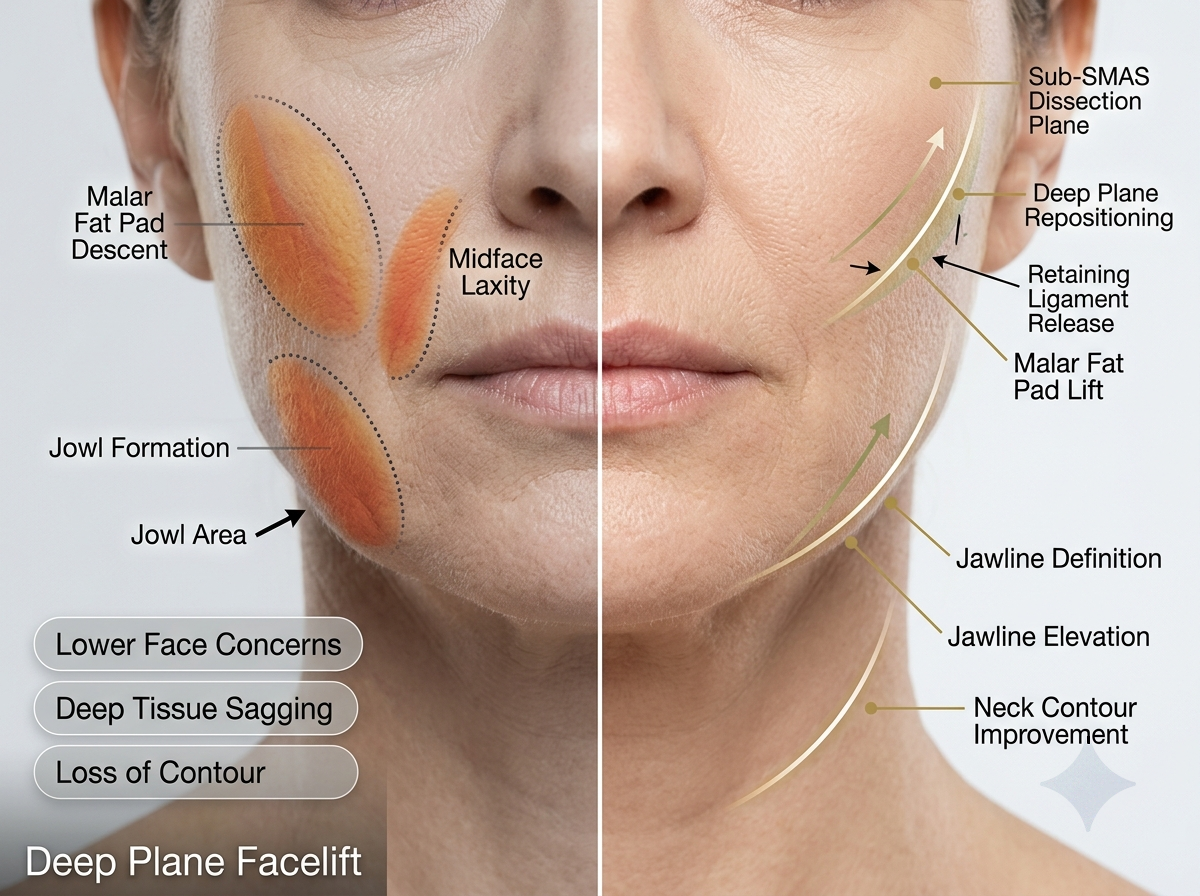
Quick answer: The deep plane facelift technique elevates the SMAS, subcutaneous fat, and skin as one composite flap rather than as separate layers. Releasing the zygomatic and masseteric retaining ligaments lets this unit move along its natural vector, repositioning descended tissue while preserving the flap’s own blood supply and avoiding tension on the skin surface itself.
The deep plane facelift is defined by how tissue is dissected and moved, not simply by the fact that it addresses deeper facial layers than skin alone. This article sets out the surgical anatomy behind the technique — the composite flap concept, the retaining ligaments released, the facial nerve anatomy that governs dissection safety, and the sequence of steps involved — for readers who want the technical detail behind the procedure.
For candidacy, recovery timelines, and cost considerations, see the facelift in Dubai guide. Full procedure information is available on the facelift page.
What Is the Composite Flap in a Deep Plane Facelift?
In a standard subcutaneous facelift, the skin is dissected away from the SMAS (Superficial Musculo-Aponeurotic System) as a separate layer, leaving the SMAS to be tightened independently through plication or imbrication. A deep plane facelift instead dissects beneath the SMAS, elevating skin, subcutaneous fat, and SMAS together as a single composite flap.
This distinction matters for two reasons:
- Vascular supply. The perforator vessels connecting the SMAS to the overlying skin remain intact within the composite flap, rather than being severed during a separate subcutaneous dissection.
- Mechanical unity. Because skin and SMAS move as one unit, the flap can be repositioned along the vector needed to correct descended tissue, rather than relying on skin tension to simulate a lift.
The composite flap concept is the anatomical basis for every other aspect of the technique discussed below.
Which Facial Retaining Ligaments Are Released, and Why?
Facial soft tissue is held in position by a series of fibrous retaining ligaments that anchor the dermis to the underlying periosteum or deep fascia. A subcutaneous or SMAS-plication facelift largely works around these ligaments; a deep plane facelift releases them directly, which is what allows the composite flap to move rather than merely stretch.
| Ligament | Anatomical location | Function | Relevance to deep plane release |
|---|---|---|---|
| Zygomatic cutaneous ligaments | Zygomatic arch / malar region | Anchor cheek skin to the zygoma | Release allows mid-face composite mobilization |
| Masseteric cutaneous ligaments | Anterior border of the masseter | Anchor lower cheek to the masseter fascia | Release allows jowl and lower-face repositioning |
| Mandibular (mandibulocutaneous) ligament | Anterior mandible | Anchor jawline skin to bone | Selectively addressed depending on jowl severity |
| Platysma-auricular ligament | Angle of mandible / neck | Anchors platysma to the deep neck fascia | Released when neck correction is combined |
Only the ligaments relevant to the individual’s pattern of descent are released — ligament release is targeted anatomical work, not a blanket dissection.
Layer-by-Layer Surgical Steps of Deep Plane Dissection
While specifics vary by anatomy and whether neck correction is combined, the deep plane technique generally follows this sequence:
- Skin incisions are marked along the temporal hairline, pre-auricular crease, and into the occipital scalp.
- A limited subcutaneous dissection is carried out only across the narrow anterior cheek margin, preserving SMAS attachment everywhere else.
- The SMAS is identified and entered, transitioning the dissection into the sub-SMAS (deep) plane.
- Sub-SMAS dissection proceeds anterior to the parotid gland, across the masseter.
- The zygomatic and masseteric cutaneous ligaments are released under direct visualization.
- The mobilized composite flap is repositioned along the vector required to correct the specific pattern of descent.
- The flap is fixed to stable points — typically the deep temporal fascia and periosteum — to carry the corrective tension internally.
- Skin is redraped over the repositioned composite flap and closed without tension, since the lift itself is already held by the internal fixation.
How Does Deep Plane Dissection Protect the Facial Nerve?
This is the anatomical question that governs why deep plane technique requires specific surgical training beyond standard facelift experience.
Over the body of the parotid gland, the facial nerve’s branches (frontal, zygomatic, buccal, and marginal mandibular) run deep to the SMAS. A dissection correctly maintained in the sub-SMAS plane over the parotid therefore stays superficial to these branches. As the branches exit the anterior border of the parotid and cross the masseter toward the mid-face, however, they become progressively more superficial — this region is treated as a defined anatomical danger zone.
Correct execution of the technique depends on:
- Precise identification of the sub-SMAS plane before crossing the anterior parotid border
- Recognition of the danger zone over the masseter, where dissection depth must be adjusted
- Direct visualization rather than blunt dissection through poorly defined tissue planes
This is why deep plane dissection is considered more technically demanding than subcutaneous or SMAS-plication facelifts, and why it is performed by surgeons with specific training in this anatomical plane. As with any surgical technique, correct execution reduces — but does not eliminate — inherent procedural risk.
Deep Plane vs. Subcutaneous Dissection: Anatomical Comparison
| Parameter | Subcutaneous facelift | Deep plane facelift |
|---|---|---|
| Dissection plane | Above the SMAS, within subcutaneous fat | Sub-SMAS, superficial to the parotid fascia |
| Tissue elevated | Skin only | Skin, subcutaneous fat, and SMAS as one composite unit |
| Flap blood supply | Random subdermal plexus | Preserved perforators linking SMAS and skin |
| Facial nerve relationship | Nerve branches lie deep to the dissection plane | Nerve branches lie deep to the plane over the parotid, closer to it over the masseter |
| Ligament handling | Ligaments largely undisturbed | Zygomatic and masseteric ligaments directly released |
| Corrective mechanism | Skin tension | Repositioned composite flap fixed internally |
This table addresses the anatomical and technical differences between the two approaches. For a comparison of candidacy, recovery timeline, and expected longevity, see the facelift in Dubai guide.
Complications Specific to Deep Plane Dissection
As with any surgical technique, deep plane facelift carries risks specific to its dissection plane and the tissue mobilized:
- Hematoma — bleeding beneath the composite flap, most often in the first 24–48 hours
- Temporary facial nerve neurapraxia — nerve stretch or bruising causing transient weakness, which typically resolves as swelling subsides
- Permanent nerve injury — rare, and associated with dissection outside the correct anatomical plane
- Contour irregularity — most often the result of incomplete ligament release rather than the composite flap technique itself
- Flap ischemia — uncommon given the preserved vascular supply of the composite flap, but a relevant consideration in smokers or previously scarred tissue
These risks, their likelihood, and mitigation are reviewed individually during a pre-operative clinical consultation; no surgical technique eliminates procedural risk entirely.
What Determines Candidacy for Composite Flap Elevation?
Composite flap elevation is not the appropriate technique for every patient. Candidacy depends on:
- The degree and pattern of mid-face and jawline descent
- Skin and soft tissue quality, including elasticity and thickness
- Any prior facial surgery affecting tissue planes or scarring
- General medical fitness for a longer operative and anaesthesia time relative to a subcutaneous or limited-incision lift
Patients with early or mild laxity are frequently better suited to a more limited technique; the anatomical assessment during consultation — not the desire for a specific named technique — determines what is appropriate.
Dr. Bouraoui Kotti, EBOPRAS-certified Consultant Plastic Surgeon at Seline Clinic, Jumeirah, Dubai, performs deep plane facelift surgery based on individual anatomical assessment. This article is provided for patient and professional education; it does not substitute for a clinical consultation.
Medical disclaimer: This article is provided for educational purposes. Suitability for surgery, technique selection, and outcomes depend on individual anatomical factors, health status, and personalized surgical planning. A consultation with a DHA-licensed Consultant is required before any procedure.
Related procedures and guides:
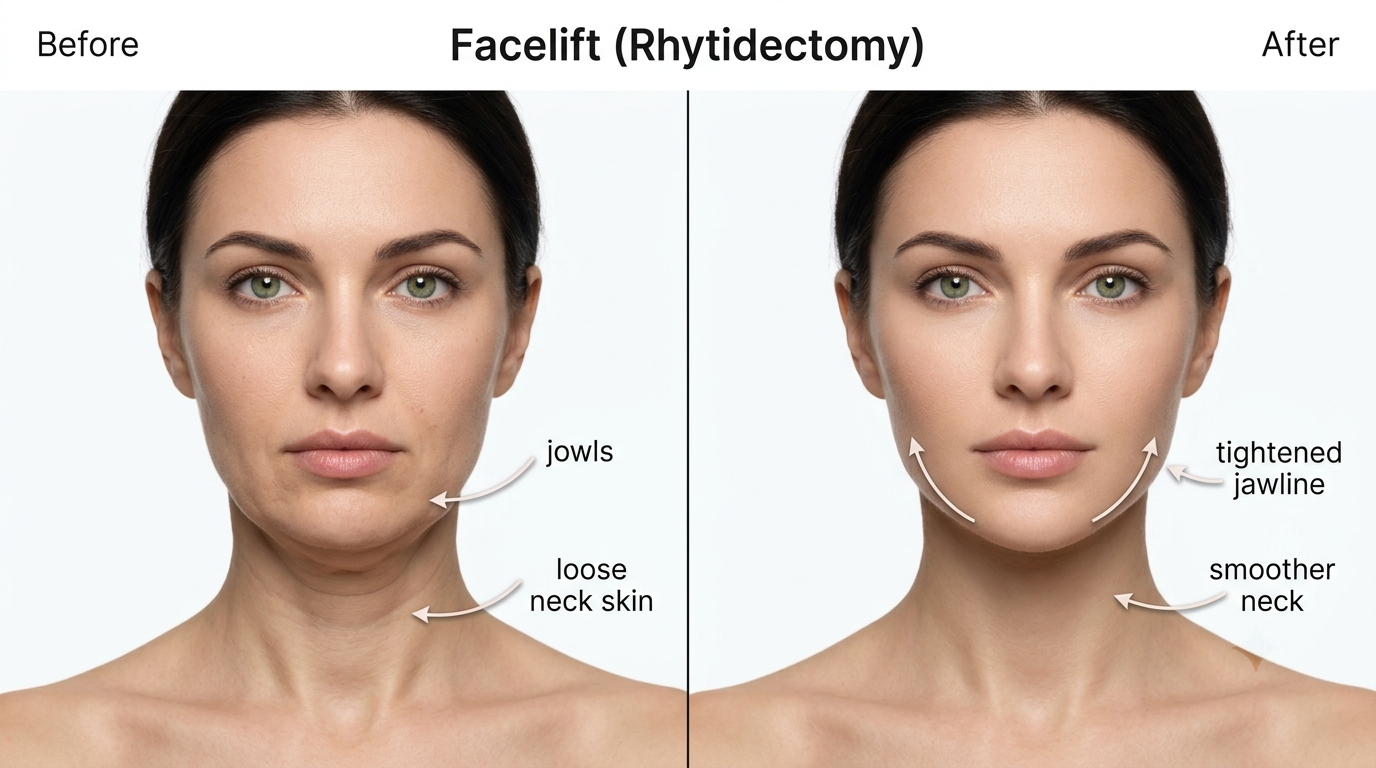
- Facelift (Rhytidectomy) — Full procedure details, candidacy, and risks
- Facelift in Dubai: Cost, Recovery & Results — Technique comparison, candidacy, and recovery timeline
- Facelift & Neck Contouring — Surgical procedure page
- Neck Lift Guide — Educational cervicoplasty overview
- Eyelid Surgery (Blepharoplasty) — Periocular rejuvenation
- Before & After Gallery — Clinical results documentation
- Book a Consultation — Private clinical assessment at Seline Clinic, Jumeirah
Frequently Asked Questions
What is a composite flap in a deep plane facelift?
A composite flap is the skin, subcutaneous fat, and SMAS elevated together as a single anatomical unit, rather than dissecting the skin and SMAS as separate layers. Because the natural attachments between these layers are preserved, the flap retains its own blood supply and can be repositioned as one structure along its original vector.
Which facial ligaments are released during deep plane facelift surgery?
The zygomatic cutaneous and masseteric cutaneous ligaments are released to mobilize the mid-face composite. When neck correction is combined with the facelift, the platysma-auricular ligament is also addressed. Releasing these retaining ligaments, rather than only tensioning the skin, is what allows descended tissue to be repositioned rather than simply pulled tighter.
How does deep plane dissection protect the facial nerve?
Over the parotid gland, the facial nerve branches run deep to the SMAS, so a correctly maintained sub-SMAS plane stays superficial to them. The branches become more superficial as they cross the masseter toward the mid-face, which is why this region is treated as a defined anatomical danger zone requiring precise plane identification and surgical experience with the technique.
Why is the deep plane technique more vascularly stable than a subcutaneous facelift?
A subcutaneous flap depends on a random subdermal blood supply, which thins as the flap is elevated. A composite flap keeps its myocutaneous perforator vessels intact because the SMAS is elevated together with the skin, supporting flap perfusion — a relevant consideration in smokers or previously operated tissue.
What determines candidacy for composite flap elevation?
Candidacy depends on the degree of mid-face and jawline descent, skin and soft tissue quality, prior facial surgery, and general medical fitness for a longer operative and anaesthesia time compared with a subcutaneous or limited-incision lift. Anatomical assessment during a clinical consultation determines whether composite flap elevation is appropriate.
What are the technique-specific risks of deep plane facelift surgery?
Documented risks include hematoma, temporary facial nerve neurapraxia, and, rarely, permanent nerve injury if the dissection plane is not correctly maintained. Incomplete ligament release can also result in residual contour irregularity. These risks are inherent to the technique and are discussed individually during pre-operative consultation.
How is the composite flap secured during deep plane facelift surgery?
The mobilized composite flap is fixed to stable points such as the deep temporal fascia and periosteum along a vector determined by the direction of tissue descent, then the skin is redraped and closed without tension. Because the lift is carried by the fixed composite flap rather than skin tension, the closure itself does not bear the corrective load.
Related Clinical Articles
Facelift Cost & Recovery Dubai | Clinical Guide
Facelift cost recovery Dubai — technique options, recovery staging, and candidacy factors for informed clinical planning.
Jun 18, 2026
Lip Lift Surgery Dubai | Reduction & Flip Guide
Lip lift surgery Dubai — Bullhorn lift, reduction, and lip flip options explained by EBOPRAS Consultant Dr. Bouraoui Kotti.
Jun 28, 2026

